Endo Belly Series Part 1: Dysbiosis, & Endotoxins, More Than Endometriosis Symptom Management
If you’ve ever wondered whether your severe bloating is “normal,” you’re not alone—because the endo belly feel is anything but typical. For those living with endometriosis, endo belly refers to a unique and often overwhelming sensation that goes far beyond the average post-meal bloat. It’s that sudden, intense swelling in your lower abdominal region that can make you look several months pregnant in just a few hours, leaving you clutching your stomach and searching for relief.
What sets the endo belly feel apart is the potential combination of severe bloating, deep abdominal pressure, and persistent pain that can radiate through your digestive tract. This isn’t just a little puffiness; it can feel like a full-on, hard-as-a-rock, distended belly that can make even loose clothing feel like spandex. Alongside the visible bloated abdomen, many experience digestive issues like constipation, diarrhea, nausea, and unpredictable bowel habits—sometimes all in the same day. The discomfort can be so intense that it disrupts your ability to work, socialize, or even rest.
Unlike typical bloating, endo belly symptoms often come with a sense of heaviness and digestive discomfort that can worsen pain throughout your menstrual cycle or after eating certain foods. The pressure and pain can be relentless, sometimes accompanied by severe stomach pain, making it difficult to take deep breaths or move comfortably. For many, the emotional toll is just as significant as the physical, impacting self-confidence and making it hard to feel at ease in your own body.
If you’re struggling with the endo belly feel, know that you’re not imagining things—this is a real, distressing part of endometriosis symptoms, and you deserve support and solutions that go beyond the usual advice for managing bloating! That’s why I wrote this series, so you can have some much better ideas of what to do besides being recommended ginger tea and crackers.
The Endo Belly Series
Now, I love really delving into the complex realities of endo-belly, and today we're going to talk about one connection of many: the endometriosis-bacteria connection. I argue it's an endo-elephant in the room, creating a lot of problems in the endo body, from symptoms to pathology. Oh, and endo belly!
It's so important, I have chapters (plural) dedicated to this topic in my endometriosis book, Heal Endo.
For now, read on to discover the connection between bacterial imbalances in the gut and endo belly. And remember, these articles are long and in-depth (not just click-bait) so sit back, relax, and take the time really read :)
And don't forget to check out my other endo belly culprit articles:
Endo lesions, cysts, or adenomyosis
Endometriosis Belly and Too many "bad" bacteria
In our gut, we have a wide variety of bacteria. Some are really helpful; we often refer to them as "good guys," and you're probably really familiar with the names of some of them, like Lactobacillus or Bifidobacteria. Other bacteria are not as helpful, and although they're not "super bad" per se (it's very normal to have a bit of them; we're not trying to eradicate them), they are still considered the bad guys when there are too many. We call these "gram-negative" bacteria, and you probably also know a few names, like E. coli or Shigella.
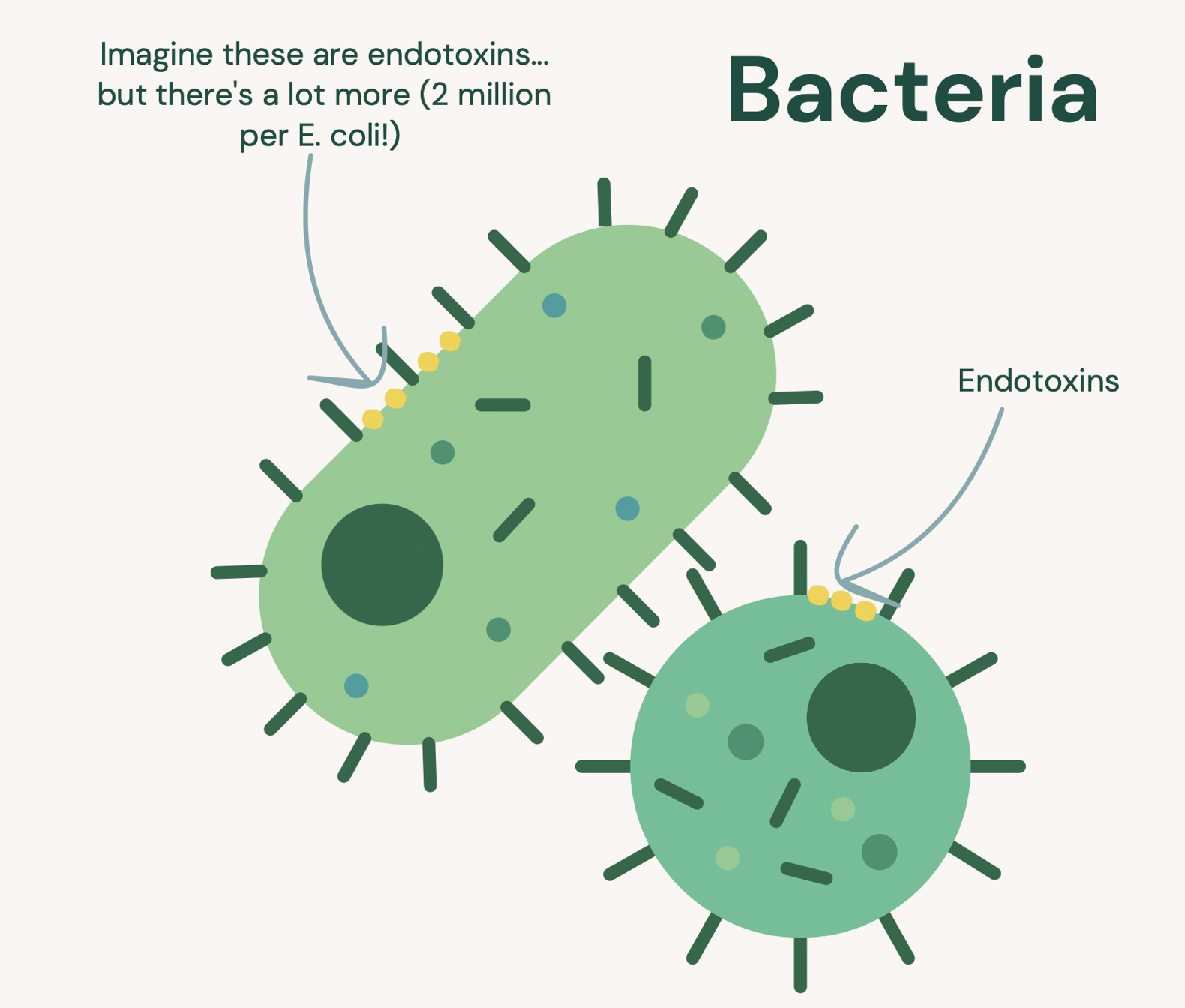
One reason these little bacteria are problematic is that they have millions of these little particles called lipopolysaccharides (LPS) or endotoxins, which are pretty gnarly little particles that reside in the outer membrane
Endotoxins are extremely immune-stimulating, a fancy way of saying your immune system HATES them and will attack them with a vengeance. This is problematic since one single bacterial cell contains around 2 million endotoxins! [1] These endotoxins are easily shed when the bacteria die or are actively growing in population size, meaning you could easily have gazillions of these molecules roaming in your intestinal tract at any given moment.
If endotoxins stay in your intestinal tract and exit via the toilet, high-five to you! If they escape into your body and end up in your blood, this is called endotoxemia—the presence of endotoxins in the blood.
If this happens, Houston, we have a problem! And guess what, Houston has found a problem in endo patients.
Endotoxins, Leaky Gut, and Endo Belly Symptoms
One reason endotoxins get into the body is thanks to leaky gut, a byproduct of gut dysbiosis that leads the intestinal tract to become damaged.
Gut dysbiosis is an imbalance within the gut microbial communities, skewing them from a favorable environment replete with diversity, nutrient production, low levels of inflammation, and wonderfully digested foods to an unfavorable condition.
This is thanks to antibiotics, medications, birth control, processed foods, stress, poor food diversity and quality, and terrible digestion, all of which breed certain types of bacterial overgrowths, many of them the gram-negative variety (they love that type of stuff). Birth control pills, in particular, are commonly used as a hormonal therapy to help manage endometriosis symptoms, regulate menstrual cycles, and potentially reduce endo belly flare-ups, though they may also have effects on gut health.
An unhealthy intestinal ecosystem can also change the localized environments that keep certain bacteria where they belong. This is how bacteria from the fecal zone (large intestine) will be able to migrate up to the small intestine and survive there, contributing to an issue called SIBO (Small Intestinal Bacterial Overgrowth).
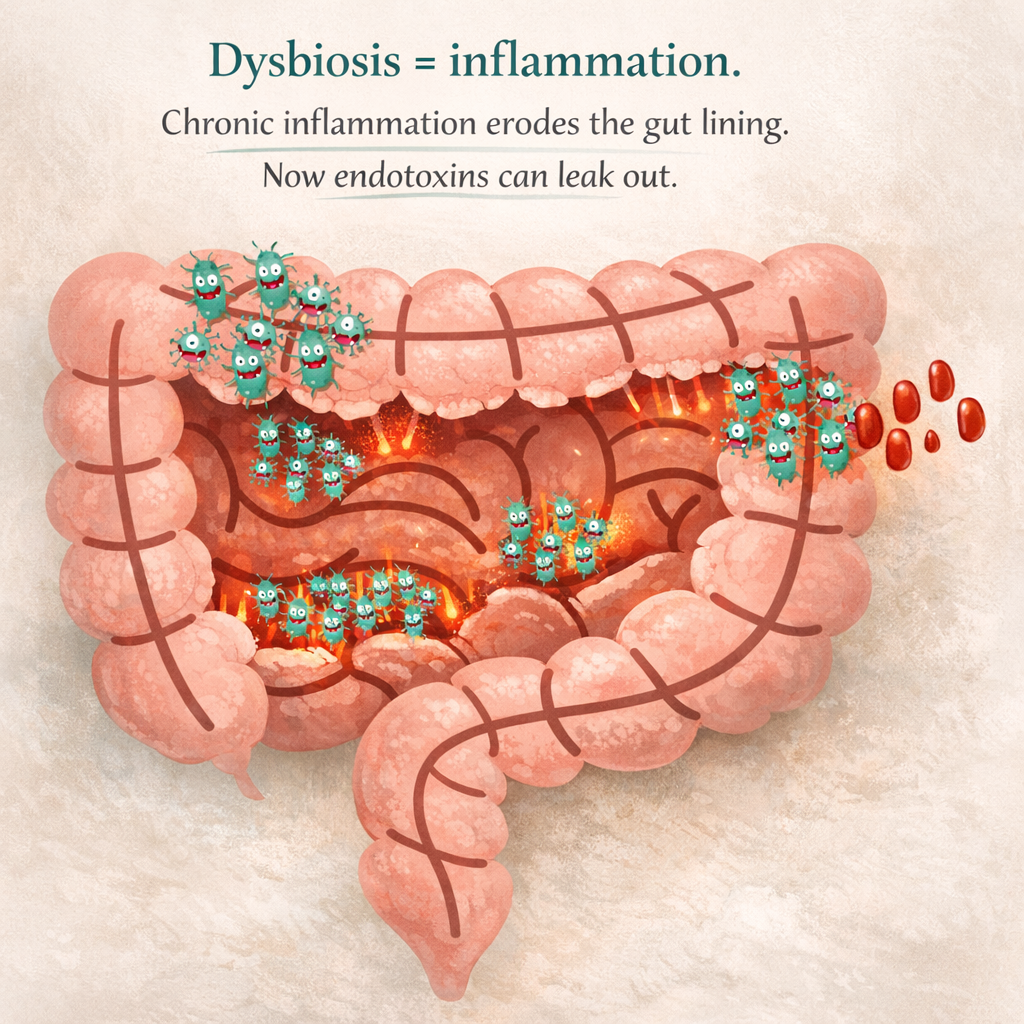
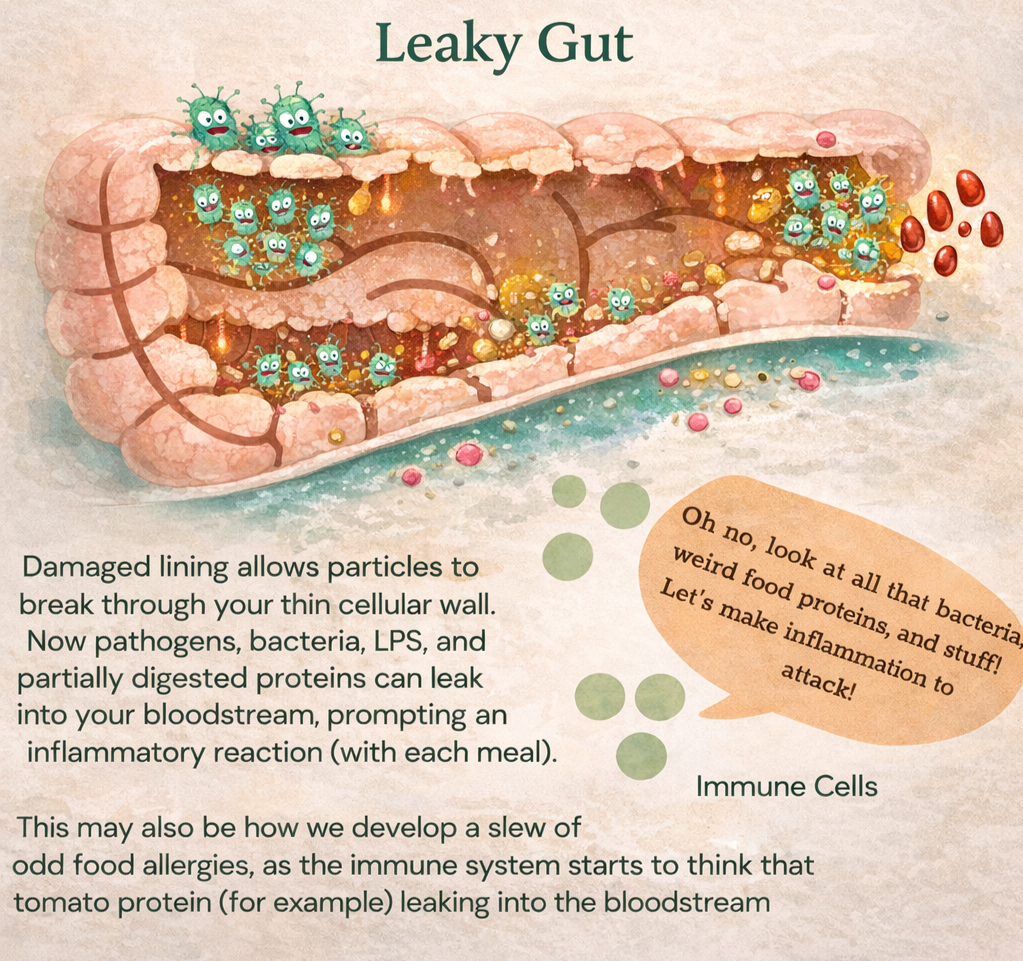
As gram-negative populations fill up the small or large intestine, replete with their millions of endotoxins per cell (!!!), the immune system will start to go BONKERS on the attack. Chronic inflammation ensues, which slowly erodes the luscious mucous lining, exposing the gut epithelial cell lining. More inflammation ensues (because those darn endotoxins keep shedding), which damages this cell lining keeping the insides of your intestinal tract from leaking out, and BOOM. You now have leaky gut.
Leaky gut is well regarded to be associated with immune dysfunction on a mass scale as your immune factors goes a bit crazy to clean up this mess — at every meal. With LPS, bacteria, undigested food particles, and more leaking into your bloodstream, better believe your immune system will start to go on the fritz.
Endometriosis, Bloated Belly, and Dysbiosis
Unfortunately, if you have endometriosis, research shows it’s highly likely that you will also have dysbiosis of the gut and reproductive tract, leaky gut, and the endotoxemia associated with it. Yup, even if you don’t have digestive issues.
In one study, researchers compared the gut microbiome of women with endo versus healthy controls, finding we all pretty much have dysbiosis. And the level of dysbiosis may correlate with disease level, as other research found women with stage 3 or 4 endo had so many gram-negative populations that they dominated their gut microbial communities (which is Bad with a capital B)! Another small study uncovered that 80% of women with endo and digestive issues were positive for SIBO. [2-4]
Early research by experts like Dr. Shanti Mohling found that a staggering 100% of endo patients studied showed signs of leaky gut [5]. Today, newer research is confirming this link even further, showing that 'tight junction' proteins like Zonulin are often haywire in the endo-body, literally leaving the door open for those millions of endotoxins to flood our system and trigger the dreaded endo belly.
Put together, this may be one reason why those with endometriosis were found to have significantly higher levels of LPS in their blood (endotoxemia) than healthy women. [6]
In other weird news, it was discovered the DNA of endo lesions is 96% similar to that of Shigella, a gram-negative fecal bacteria. Shigella can invade the large intestinal mucosa, causing inflammation and tissue damage until leaky gut occurs—where Shigella may be able to leak out. This has led researchers to propose that this bacteria may be more easily able to escape right next to the Pouch of Douglas (where the start of endometriosis is often found), triggering a cascade of inflammation and changes in the pelvic immune environment associated with endometriosis. [7]
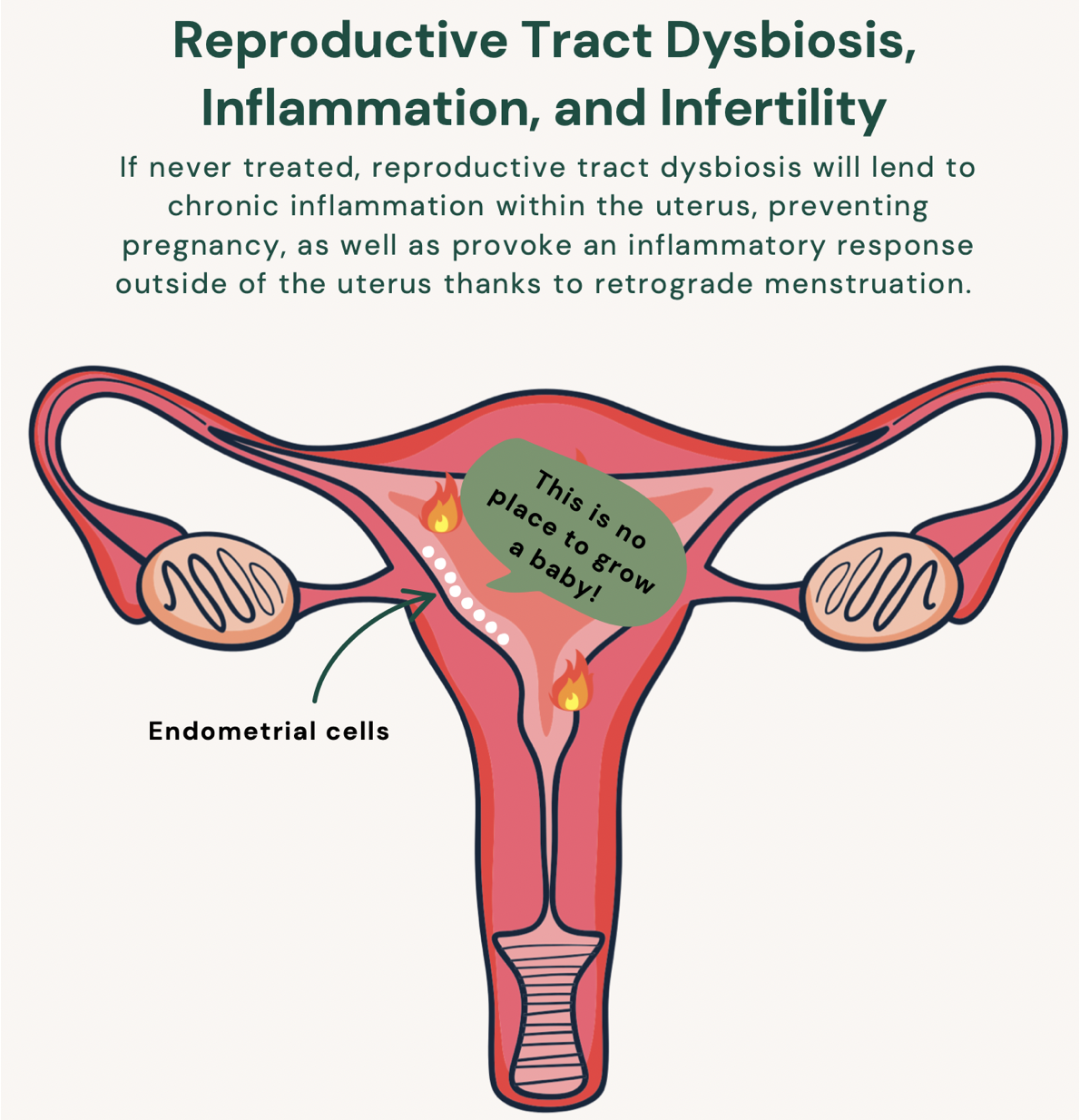
But dysbiosis and its leaky counterpart endotoxemia aren’t limited to the gut. Gram-negative bacteria are also shown to proliferate throughout the reproductive and genital tract, where they can escape through a “leaky uterus” (a word I totally just made up to describe the totally normal process of retrograde menstruation).
For example, endo sufferers have been observed to have the following: [8]
A significantly altered cervical and uterine microbiome;
More Strep in the cervical mucus (a gram-negative bacteria)
Four to six times more E. coli in the menstrual blood (more gram-negative bacteria); and
Higher levels of Streptococcus and E. coli in the endometrium (omg this is a lot of gram-negative bacteria)
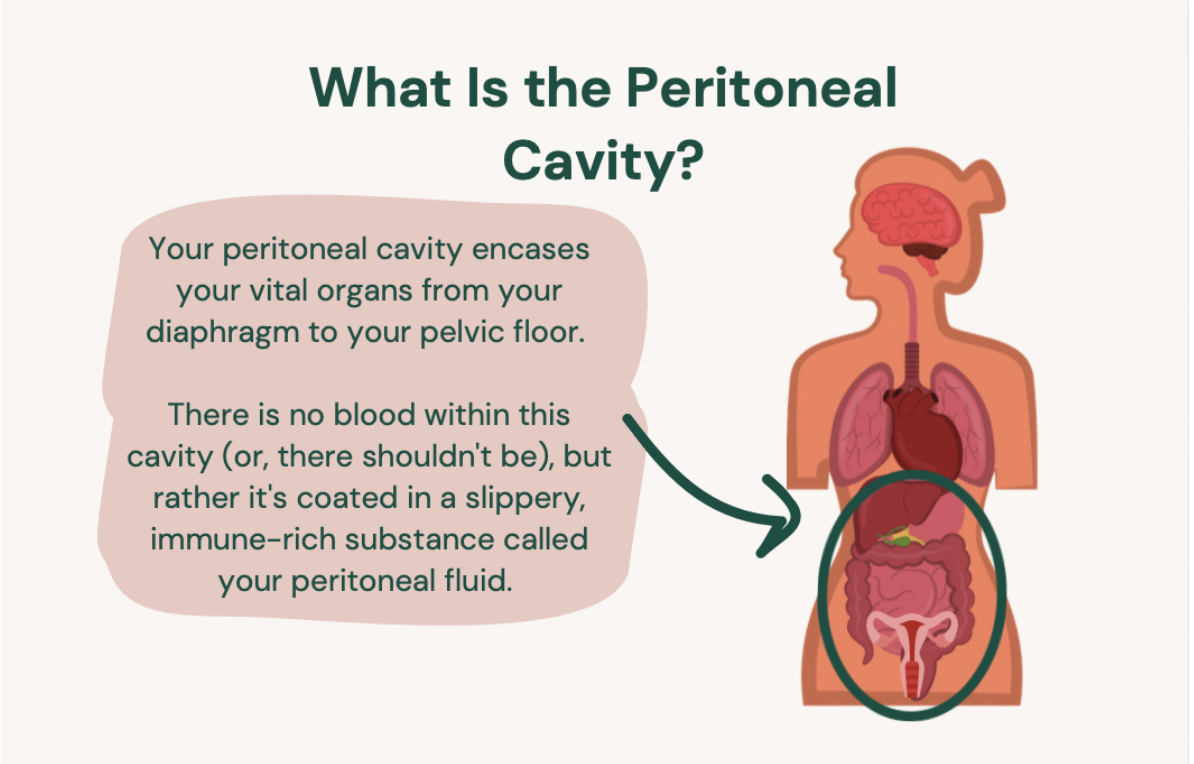
Now, thanks to retrograde menstruation—a totally natural process that may affect all women—hundreds of billions of endotoxins can leak into the peritoneal cavity and bloodstream with each period. This may be how women with endo were shown to have significantly higher levels of gram-negative bacteria in the peritoneal cavity, including one known for its ability to provoke an intense inflammatory response: Pseudomonas. Pseudomonas was also found to actually colonize the endo lesions of women with deep infiltrating endometriosis (an advanced form of the disease that develops after years of unchecked, intense inflammation)—talk about provoking inflammation. [9, 10]
Endo sufferers were also found to have a host of other gram-negative bacteria in the peritoneal cavity associated with urinary and genital infections, as well as have a 3x higher likelihood of developing endometriosis if you have Pelvic Inflammatory Disease (an infection of the peritoneal cavity)—why research is proposing genital and reproductive tract infections could be a co-factor causing endometriosis. [11]
Putting gut and reproductive tract dysbiosis together, we can start to see how women with endometriosis have LPS just about everywhere, from the gut to the cervix and uterus, to the peritoneal cavity, and in the blood.[12, 13]
Houston, are you seeing the problem?
HOUSTON TO IMMUNE SYSTEM “DESTROY THE ENDOTOXINS!”
Even a small amount of endotoxin can trigger the immune system to send lots of inflammatory immune factors to address this big-bad issue. So, when confronted with a lot of LPS, you can imagine your immune system will start WW3 to get rid of it. This is how endotoxins appear to be strongly linked to endometriosis-related inflammation, whether systemic or at the lesion site.
When looking at the localized environment (in the peritoneal cavity), LPS stimulates the immune system to send many of the exact immune players that foster endo to arrive on the scene—in this case, inflammatory immune factors mistakenly aid in the establishment and progression of endometriosis. This is why bacterial contamination may even be associated with the onset of endometriosis for some of us (remember, not all of us had our endo develop the same way), by triggering a landslide of inflammation. [14,15]
When talking about scar tissue and adhesions, you may also warily eye those endotoxins since chronic inflammation itself is what creates these issues. That’s right, it’s not endo lesions directly that cause scar tissue and adhesions; it’s the immune response that won’t turn off! Inflammation is gnarly—like bombs exploding cells kind of gnarly—so if it doesn’t stop, that damage will literally damage you. “Oops” said your immune system, as it scars and burns your organs. And one reason it’s not turning off may be due to the LPS that keeps coming with every meal or period. Gulp.
But remember, endotoxemia is found in systemic blood levels of endo patients as well. That means it’s circulating everywhere, stimulating your immune system to inflame the whole body. This is why endotoxemia is associated with chronic, low-grade systemic inflammation and continuous immune up-regulation. And FYI, to help connect the dots, endometriosis is known for chronic, low-grade inflammation and continuous immune up-regulation as well…
Immune stimulation and up-regulation like this, without end, is associated with just about every chronic disease in the book, as well as the symptoms of inflammation that accompany it: migraines, headaches, chronic fatigue, depression, anxiety, joint pain, skin issues, insomnia, and more. Yes, all “mysterious” issues many of us with endo suffer from.
NOT TO MENTION THE IMMUNE SYSTEM IS TRAINED (OR MISLED) BY GUT BACTERIA IN THE GUT
As I write about in my book, the immune system is acting a bit insane in the endo-body by establishing endo lesions and then letting them stay—and some of the reason why may be thanks to dysbiosis itself! The gut is actually the home of the immune system, where many immune cells are grown and trained in how to behave through a bacteria-immune conversation. When bacteria become imbalanced (dysbiosis) the conversation can quickly become skewed, directly influencing how immune components behave. This is why leaky gut and dysbiosis are associated with immune dysfunction. [16]
Specifically for those of us with endometriosis, gut dysbiosis may directly train our immune cells to misbehave in specific ways that support endometriosis establishment, growth, progression, and inability to clean up this mess. This includes immune cells unable to “see” or clean up endometriotic debris as they should, the immune system misbehaving by inducing inflammation in the pelvic cavity, increasing prostaglandin levels (which contributes to pain), and supporting the rooting down of endo lesions.[17]
[If you want all the nerdy science make sure to read my book, I have a whole appendix on this topic]
In short, it means your dysbiosis may be directly responsible for aiding the immune dysfunction ravaging your pelvis (or wherever your endo lesions are) as well as contributing to all the haywire symptoms that come along with immune dysfunction: chronic allergies, skin problems, hypothyroid, celiac, chronic fatigue, fibromyalgia, joint pain, and frequent headaches—many symptoms shared by endometriosis sufferers.
DYSBIOSIS, ENDOMETRIOSIS, GASTROINTESTINAL SYMPTOMS, AND INFERTILITY
Reproductive tract dysbiosis may be a big factor when it comes to infertility, something that up to a third of women with endo may deal with at some point (of note, “infertility” does not mean you can never have children, but rather refers to someone who has tried to conceive for over a year with no success). In fact, one study demonstrated that 42.3 percent of women with endometriosis and infertility issues also had chronic endometritis, an acute and prolonged infection of the endometrium lining. Endometritis is associated with recurrent miscarriages, as well as with the same strains of bacteria associated with endometriosis. Because nearly half of infertile endo patients may be dealing with this infection, I believe it’s important to investigate. In this case, a simple antibiotic treatment could dramatically improve fertility.[18,19]
Even if you don't have a diagnosable infection, you may have a subclinical infection (basically some serious dysbiosis), as 81.5 percent of women with endo were shown to have some degree of gram-negative overgrowths in the uterus. These bacteria produce never ending amounts of LPS, which can directly cause endometrial or tubal damage, prevent implantation, reduce sperm motility, and even kill sperm. In an IVF study analyzing successful outcomes, women with less LPS in the reproductive tract were much more likely to have a successful embryo transfer than those with more LPS. [20,21]
Yet, few endo-folk I’ve talked to have been told about the connection, even as they start on round 4 or 5 of IVF (do you know how expensive IVF is?? Or how heartbreaking this is??). Yes, healing the microbiome is a top priority for infertility cases.
MEND THE MICROBES TO MANAGE ENDOMETRIOSIS
Addressing dysbiosis at the gut and reproductive tract level may help you directly treat some of your worst endo symptoms, if not your endo lesions themselves. Just as we see LPS and pathogenic bacteria fostering endometriosis, so too do we see the beginnings of research uncovering the relationship between the reversal of dysbiosis and the regression of endometriosis lesions.
In a fascinating 2019 study, researchers treating endo and dysbiosis-induced mice with antibiotics observed their lesions shrink to one-fifth the size while inflammatory immune factors related to endo were all reduced. [22]
In another study, mice again were induced with endo and dysbiosis. Half of these mice were left alone, and the other half were supplemented with a gut-healing nutrient called butyrate known to repair the intestinal barrier. What they found was that the untreated mice developed larger endo lesions, while the mice supplemented with butyrate developed fewer and much smaller lesions, again demonstrating the endo-gut cross-talk. [23]
Even more recently, researchers used mice without a microbiome (yes, they can do this in a lab) and and induced endo. They then inserted gut microbiomes into these mice, giving half a fecal transplant from other endo-induced mice that did have a microbiome, and the other half a microbiome from healthy mice. What they found was that when given the microbiome associated with endo, lesions grew and progressed, while the mice given a “healthy control” microbiome did not have any endo progression, demonstrating again just how strong the endo-gut crosstalk is.[24]
We also see research showing that substances with helpful antimicrobial properties such as berberine may be able to positively impact endo. Berberine is a natural antimicrobial compound with an affinity for LPS which has been shown to reduce the inflammatory components associated with both LPS and endo. It’s even been shown to increase endometriosis cell death and reduce the proliferation and invasiveness of adenomyosis tissue (when endometrial tissue grows into the muscular wall of the uterus) by up to 60 percent! [25,26]
In humans, we don’t have any studies just yet that examine how endo behaves when bacteria is addressed (soon we will thanks to advanced imaging, though!). However, we do know through human studies that endometriosis lesions indeed can stabilize or regress when inflammation is stopped—which is the whole point of my book, btw. [27,28]
Since chronic inflammation and immune dysfunction drive endometriosis, and dysbiosis and endotoxemia drive chronic inflammation and immune dysfunction, we absolutely need to get rid of the endotoxemia and the dysbiosis driving it in order to heal fully.
THE BIG ENDO BELLY AND ENDOMETRIOSIS PICTURE
Thus, to address endometriosis as a disease and support remission, we need to address this dysbiosis and endotoxemia head-on. To do so, you will need to:
Honesty, I recommend starting with the basics of diet and lifestyle if you have not already. Addressing nutriton, sleep, stress, and movement alone can have dynamic changes in the gut microbiome.
Next up, test for the specific type of dysbiosis you have, and treat it to get rid of it if needed. This may be done in both the gut and reproductive tract. I will talk about this more in the coming posts. For now, if you’re interested, check here to see some of my fav dysbiosis un-covering tools, and read here and here about uncovering reproductive tract dysbiosis)
Heal your digestive capabilities to starve bacteria of poorly digested sugars. (some info on that here, and also lots in my Endo-Belly Ebook)
Restore a healthy microbiome community, including replacing any strains that may be clinically missing from the gut (allowing pathogens to take up place).
Restore the gut mucous lining that prevents a leaky gut from happening in the first place.
Heal the gut epithelial lining, which allows endotoxins to sneak through.
A gut healing process is no short journey. It can take 6 months to 2 years, depending on a patient’s severity. But I’m excited to be talking about this stuff over the coming posts because I do believe many of us are tired of being told to eat more fiber and drink more water to “fix” our gut issues when there’s perhaps something else really clinically significant going on.
Further Reading
2 Svensson, A., Brunkwall, L., Roth, B., Orho-Melander, M., & Ohlsson, B. (2021). Associations Between Endometriosis and Gut Microbiota. Reproductive sciences (Thousand Oaks, Calif.), 28(8), 2367–2377. https://doi.org/10.1007/s43032-021-00506-5
3 Ata, B., Yildiz, S., Turkgeldi, E., Brocal, V. P., Dinleyici, E. C., Moya, A., & Urman, B. (2019). The endobiota study: Comparison of vaginal, cervical and gut microbiota between women with stage 3/4 endometriosis and healthy controls. Scientific Reports, 9(1), 2204. https://doi.org/10.1038/s41598-019-39700-6
4 Mathias, J. R., Franklin, R., Quast, D. C., Fraga, N., Loftin, C. A., Yates, L., & Harrison, V. (1998). Relation of endometriosis and neuromuscular disease of the gastrointestinal tract: New insights. Fertility and Sterility, 70(1), 81–88. https://doi.org/10.1016/s0015-0282(98)00096-x
5 https://www.endofound.org/is-there-a-link-between-leaky-gut-and-endo-this-researcher-thinks-so
6 Viganó, D., Zara, F., Pinto, S., Loddo, E., Casula, L., Soru, M. B., D'Ancona, G., D'Alterio, M. N., Giuliani, C., Angioni, S., & Usai, P. (2020). How is small bowel permeability in endometriosis patients? a case control pilot study. Gynecological endocrinology : the official journal of the International Society of Gynecological Endocrinology, 36(11), 1010–1014. https://doi.org/10.1080/09513590.2020.1766440
7 Kodati, V. L., Govindan, S., Movva, S., Ponnala, S., & Hasan, Q. (2008). Role of Shigella infection in endometriosis: a novel hypothesis. Medical hypotheses, 70(2), 239–243. https://doi.org/10.1016/j.mehy.2007.06.012
8 Khan, K. N., Kitajima, M., Hiraki, K., Yamaguchi, N., Katamine, S., Matsuyama, T., Nakashima, M., Fujishita, A., Ishimaru, T., & Masuzaki, H. (2010). Escherichia coli contamination of menstrual blood and effect of bacterial endotoxin on endometriosis. Fertility and Sterility, 94(7), 2860–2863.e33. https://doi.org/10.1016/j.fertnstert.2010.04.053; Khan, K. N., Fujishita, A., Kitajima, M., Hiraki, K., Nakashima, M., & Masuzaki, H. (2014). Intra-uterine microbial colonization and occurrence of endometritis in women with endometriosis. Human Reproduction (Oxford, England), 29(11), 2446–2456. https://doi.org/10.1093/humrep/deu222; Koninckx, P. R., Ussia, A., Tahlak, M., Adamyan, L., Wattiez, A., Martin, D. C., & Gomel, V. (2019). Infection as a potential cofactor in the genetic-epigenetic pathophysiology of endometriosis: A systematic review. Facts, Views & Vision in ObGyn, 11(3), 209–216.
9 Huang, L., Liu, B., Liu, Z., Feng, W., Liu, M., Wang, Y., Peng, D., Fu, X., Zhu, H., Cui, Z., Xie, L., & Ma, Y. (2021). Gut Microbiota Exceeds Cervical Microbiota for Early Diagnosis of Endometriosis. Frontiers in cellular and infection microbiology, 11, 788836. https://doi.org/10.3389/fcimb.2021.788836
10 Hernandes, C., Silveira, P., Rodrigues Sereia, A. F., Christoff, A. P., Mendes, H., Valter de Oliveira, L. F., & Podgaec, S. (2020). Microbiome Profile of Deep Endometriosis Patients: Comparison of Vaginal Fluid, Endometrium and Lesion. Diagnostics (Basel, Switzerland), 10(3), 163. https://doi.org/10.3390/diagnostics10030163
11 Koninckx, P. R., Ussia, A., Tahlak, M., Adamyan, L., Wattiez, A., Martin, D. C., & Gomel, V. (2019). Infection as a potential cofactor in the genetic-epigenetic pathophysiology of endometriosis: a systematic review. Facts, views & vision in ObGyn, 11(3), 209–216.
12 Viganó, D., Zara, F., Pinto, S., Loddo, E., Casula, L., Soru, M. B., D'Ancona, G., D'Alterio, M. N., Giuliani, C., Angioni, S., & Usai, P. (2020). How is small bowel permeability in endometriosis patients? a case control pilot study. Gynecological endocrinology : the official journal of the International Society of Gynecological Endocrinology, 36(11), 1010–1014. https://doi.org/10.1080/09513590.2020.1766440
13 Koninckx, P. R., Ussia, A., Tahlak, M., Adamyan, L., Wattiez, A., Martin, D. C., & Gomel, V. (2019). Infection as a potential cofactor in the genetic-epigenetic pathophysiology of endometriosis: A systematic review. Facts, Views & Vision in ObGyn, 11(3), 209–216.
14 Khan, K. N., Fujishita, A., Hiraki, K., Kitajima, M., Nakashima, M., Fushiki, S., & Kitawaki, J. (2018). Bacterial contamination hypothesis: a new concept in endometriosis. Reproductive medicine and biology, 17(2), 125–133. https://doi.org/10.1002/rmb2.12083
15 Khan, K. N., Fujishita, A., Hiraki, K., Kitajima, M., Nakashima, M., Fushiki, S., & Kitawaki, J. (2018). Bacterial contamination hypothesis: a new concept in endometriosis. Reproductive medicine and biology, 17(2), 125–133. https://doi.org/10.1002/rmb2.12083
16 Laschke, M. W., & Menger, M. D. (2016). The gut microbiota: A puppet master in the pathogenesis of endometriosis? American Journal of Obstetrics and Gynecology, 215(1), 68.e1–68.e4. https://doi.org/10.1016/j.ajog.2016.02.036; Wu, H. J., & Wu, E. (2012). The role of gut microbiota in immune homeostasis and autoimmunity. Gut Microbes, 3(1), 4–14. https://doi.org/10.4161/gmic.19320
17 Emani, R., Alam, C., Pekkala, S., Zafar, S., Emani, M. R., & Hänninen, A. (2015). Peritoneal cavity is a route for gut-derived microbial signals to promote autoimmunity in non-obese diabetic mice. Scandinavian Journal of Immunology, 81(2), 102–109. https://doi.org/10.1111/sji.12253
18 Cicinelli, E., Trojano, G., Mastromauro, M., Vimercati, A., Marinaccio, M., Mitola, P. C., Resta, L., & de Ziegler, D. (2017). Higher prevalence of chronic endometritis in women with endometriosis: A possible etiopathogenetic link. Fertility and Sterility, 108(2), 289–295.e1. https://doi.org/10.1016/j.fertnstert.2017.05.016
19 Cicinelli, E., Matteo, M., Tinelli, R., Pinto, V., Marinaccio, M., Indraccolo, U., De Ziegler, D., & Resta, L. (2014). Chronic endometritis due to common bacteria is prevalent in women with recurrent miscarriage as confirmed by improved pregnancy outcome after antibiotic treatment. Reproductive Sciences (Thousand Oaks, Calif.), 21(5), 640–647. https://doi.org/10.1177/1933719113508817
20 Khan, K. N., Fujishita, A., Kitajima, M., Hiraki, K., Nakashima, M., & Masuzaki, H. (2014). Intra-uterine microbial colonization and occurrence of endometritis in women with endometriosis†. Human reproduction (Oxford, England), 29(11), 2446–2456. https://doi.org/10.1093/humrep/deu222
21 Deb, K., Chatturvedi, M. M., Jaiswal, Y. K. (2004). Gram-negative bacterial endotoxin- induced infertility: A birds eye view. Gynecologic and Obstetric Investigation, 57, 224-232. https://www.doi.org/10.1159/000076761
22 Chadchan, S. B., Cheng, M., Parnell, L. A., Yin, Y., Schriefer, A., Mysorekar, I. U., & Kommagani, R. (2019). Antibiotic therapy with metronidazole reduces endometriosis disease progression in mice: A potential role for gut microbiota. Human Reproduction (Oxford, England), 34(6), 1106–1116. https://doi.org/10.1093/humrep/dez041
23 Chadchan, S. B., Popli, P., Ambati, C. R., Tycksen, E., Han, S. J., Bulun, S. E., Putluri, N., Biest, S. W., & Kommagani, R. (2021). Gut microbiota-derived short-chain fatty acids protect against the progression of endometriosis. Life Science Alliance, 4(12), e202101224. https://doi.org/10.26508/lsa.202101224
24 Chadchan, S.B., Naik, S.K., Popli, P. et al. Gut microbiota and microbiota-derived metabolites promotes endometriosis. Cell Death Discov. 9, 28 (2023). https://doi.org/10.1038/s41420-023-01309-0
25 Gu, Y., & Zhou, Z. (2021). Berberine inhibits the proliferation, invasion and migration of endometrial stromal cells by downregulating miR‑429. Molecular medicine reports, 23(6), 416. https://doi.org/10.3892/mmr.2021.12055
26 Liu, L., Chen, L., Jiang, C., Guo, J., Xie, Y., Kang, L., & Cheng, Z. (2017). Berberine inhibits the LPS-induced proliferation and inflammatory response of stromal cells of adenomyosis tissues mediated by the LPS/TLR4 signaling pathway. Experimental and Therapeutic Medicine, 14(6), 6125–6130. https://doi.org/10.3892/etm.2017.5316
27 Evers, J.L.H. (2013). Is adolescent endometriosis a progressive disease that needs to be diagnosed and treated? Human Reproduction, 28(8), 2023. https://doi.org/10.1093/humrep/det298
28 Fuentes, A, Escalona, J, Céspedes, P, Espinoza, A, Johnson, MC. (2014). Prevalencia de la endometriosis en mujeres sometidas a esterilización quirúrgica laparoscópica en un hospital de Santiago de Chile [Prevalence of endometriosis in 287 women undergoing surgical sterilization in Santiago Chile]. Rev Med Chil, 142(1), 16-19. Spanish. https://doi.org/10.4067/S0034-98872014000100003
Endo Belly FAQs
What is Endo Belly? Endo belly is a distressing but not commonly discussed symptom of endometriosis, characterized by severe abdominal bloating, severe swelling, and painful bloating that can cause discomfort, pain, and pressure in the abdomen, pelvis, and/or back. The swelling can fluctuate throughout the day and can worsen during certain phases of the menstrual cycle, especially just before or during your period.
What does it feel like? Many women with endo belly report feeling like they look pregnant due to the distended abdomen, but this is not true weight gain—rather, it is due to inflammation, fluid retention, and digestive issues. Endo belly is often accompanied by other gastrointestinal symptoms, such as constipation, diarrhea, and painful bowel movements, and can overlap with conditions like irritable bowel syndrome (IBS) and other gastrointestinal symptoms.
Do lesions contribute? They can! The inflammation is caused by endometrial-like tissue (different than endometrial tissue) growing on or near the intestines, which irritates the digestive system and can disrupt gut bacteria, leading to digestive discomfort and bloating. Trapped blood and fluid retention can also contribute to swelling and discomfort.
Are other factors involved? Totally, it's why I have many articles on endo belly (if only it was so straighforward!). Endometriosis and endo belly often involve hormonal and metabolic changes, as well as increased nervous system sensitivity, which can worsen symptoms. Food intolerances and inflammatory foods like gluten, dairy, and processed sugars can worsen symptoms, so keeping a food diary can help identify foods that trigger or reduce endo belly. Management strategies to reduce endo belly and ease bloating include adopting an anti-inflammatory diet rich in healthy fats and foods with anti-inflammatory properties, staying well-hydrated, engaging in gentle exercise (such as walking or yoga), practicing deep belly breathing and meditation, and using pelvic floor therapy.
Stress management techniques like mindfulness and yoga are important, as stress can worsen symptoms. Using heat pads or heating pads can provide immediate relief for abdominal pain and cramps, while gentle abdominal massage techniques and over-the-counter digestive aids may help reduce gas and nausea.
When should I find a specialist? Identifying the underlying cause of symptoms and consulting with an endometriosis specialist is crucial for advanced treatment options, including medications such as anti-inflammatory medicines, hormonal therapies (like birth control pills and gonadotropin releasing hormone drugs), and laparoscopy—the gold standard for diagnosis and removal of lesions or scar tissue.
Will helping my endo help my endo belly? Maybe. Managing the factors that influence endometriosis can also help alleviate symptoms of endo belly. Things like regular gentle exercise can reduce pain over time by improving blood flow and reducing stress, for example. While exact cause of endo belly will be different for everyone, it often involves inflammation, core function, pelvic floor, hormonal and metabolic changes, fluid retention, gut bacteria imbalances, and nervous system sensitization. Yes, lots of things :)